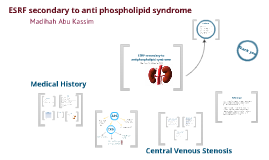
CVS
Transcript: Central Venous Stenosis ARF requiring HD How can we help? APS ~Anti phospholipid syndrome – 2 DVTs ~Digital vasculitis – 1989 ~Catastrophic anti phospholipid syndrome – 1998/9 ~ARF requiring HD – 1999 ~Heparin induced thrombocytopenia – 1999 ~Recurrent biliary sepsis 2o to CBD stricture – multiple ERCPs for dilatation & stenting ~Hepatico-jejunostomy with cholecystectomy – 2006 ~Retro uterine haemorrhage – ruptured fallopian tube – 1998 ~Previous recurrent small bowel obstruction 2o adhesion ~Grand mal seizure with left occipital infarct on CT - 1999 ~Non transmural MI with moderate to severe LV dysfunction ~Hypertension – 2002 ~Decline in renal function, assoc with presumed intra abdominal sepsis – 2010 ~Central stenosis with recurrent plasty of left brachiocephalic vein, recurrent venopasties every 6-8 weeks ~Chronic subdural haematoma – 2011 ~Calciphylaxis with lesion on shin – 2011/2 Allergies: Heparin, ciprofloxacin, livofloxacin ESRF secondary to antiphospholipid syndrome Arthritis in siblings "Dead" Left hand Common problem in the management of HD patient Prevalence: 25-40% among HD population (Kundu, 2010) Disrupts the vascular access circuit Higher risk with previous central line placement Recurrent venoplasties are stressful to Miss BP Post-traumatic stress disorder (PTSD) Miss BP 46 year old Psychotherapist Kidney diagnosis: ESRF secondary to anti-phospholipid syndrome (APS) On haemodialysis (HD) for 18 months DH Ruptured fallopian tube ESRF secondary to anti phospholipid syndrome FH Reference Central Venous Stenosis (CVS) Madihah Abu Kassim, CP2 Kundu, S (2010) Central venous disease in hemodialysis patients: prevalence, etiology and treatment. [The journal of Vascular Access, 2010; 11: 1-7] Haage, P, Vorweck, D, Piroth W, Schuermann, K, Guenther, RW (1999) Treatment of hemodialysis-related central venous stenosis or occlusion: results of primary Wallstent placement and follow-up in 50 patients. [Radiology; 212. 175-180] Central Venous Stenosis (CVS) Options for Miss BP Calciphylaxis CKD Percutaneous transluminal angioplasty High technical success rate High recurrence rate multiple intervention (stressful) Create fistula on the Right side Risk of Right hand “dying” Surgical bypass procedure Reserved if PTA fails Associated with high morbidity & mortality Kidney transplant Currently no living donor High risk of rejection SH Thank you Subdural haematoma Madihah Abu Kassim PMH CKD patients often have other co-morbidities Central venous stenosis is a common problem in management of chronic HD patient First line therapy for CVS is PTA Biopsychosocial approach for management of patients with CKD/ESRF Conclusion Background Medical History Lives alone (with her dog) Works from home Good friends around Medically: Sedatives & anxiolytics prior to procedure ?GA – high risk Psychologically: Systemic desensitisation Hypnosis